


by Six Month Smiles, on 1/12/22 7:49 AM

Six Month Smiles is proud to announce a new advancement in the fight to relieve pressure points and add stability for patients experiencing grinding issues and TMJ disorders. Six Month …
Read Moreby Six Month Smiles, on 1/5/22 10:23 AM

The term "new year, new me" has become such a cliche through the years. But like most popular cliches, it's grounded in truth. For any good Dentist, a new year …
Read Moreby Umair Ahmed, on 9/29/21 12:03 PM

Interproximal reduction (IPR) guidance for all planned cases, be they aligners or clear braces, is generated on a dental computer aided-drafting, CAD, system. Six Month Smiles utilizes your submitted scans …
Read Moreby Dr. Jorge Perez, on 6/8/21 7:00 PM

In the second part of this series, I will review examples of movements that may require refinement and why. I will also provide tips on how to avoid a refinement …
Read Moreby Six Month Smiles, on 3/16/21 11:40 AM

4 Training Options, 1 Common Goal Within the Six Month Smiles Guided Orthodontic universe, general dentists have the option of treating patients with Clear Braces, Invisible Aligners or both with …
Read Moreby Six Month Smiles, on 3/16/21 11:37 AM
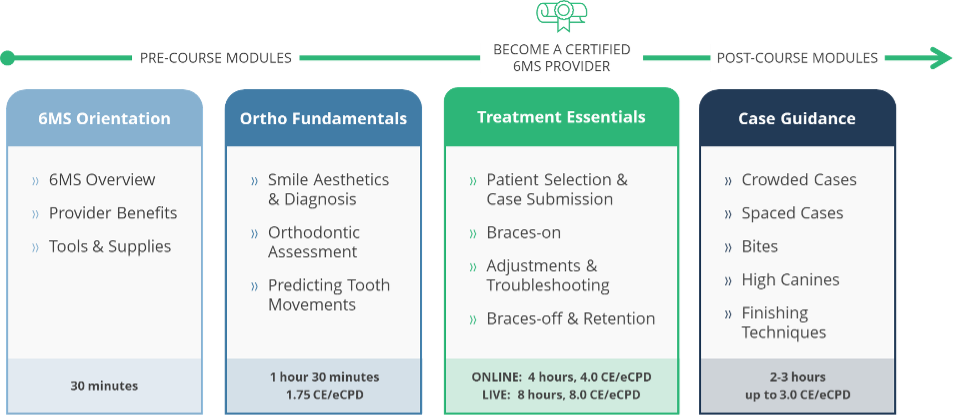
The New World and What That Means for Provider Training The world is changing, and so is Six Month Smiles! We understand that travel restrictions and social distancing have made …
Read Moreby Dr. Jorge Perez, on 2/9/21 1:07 PM
Wherever your clear aligner learning curve or experience is, I trust that at some point you have experienced somehow the need for refinement. What is a Refinement? Refinement in clear …
Read Moreby Perry Lowe, on 12/14/20 3:34 PM

There's certainly nothing in recent memory that compares to the challenges of 2020. Not only has everyone been impacted in different ways --personally and professionally-- we are likely to feel …
Read Moreby Six Month Smiles, on 12/14/20 3:24 PM

Many of you know, but some will be surprised to hear that as a Six Month Smiles Provider you are never, EVER charged for your case until it is SHIPPED …
Read Moreby Solution Reach, on 11/16/20 12:34 PM

Patients who no-show are a year-round frustration, but that frustration is compounded during the busy holiday season (and don't even mention the complications COVID has added to this!). Knowing what …
Read More(866) 957-7645 (US)
001 585 594 0606 (International)